Exkurs über die Erfolgsrate der Operation bei Verwachsungen
Firstly, physicians see adhesions, adhesion pain, adhesion causes and adhesion surgery completely differently to lay people.
There is a huge gap between patient education and field work WITH patients. To this end EndoGyn created a site to exchange views, for discussion, to educate, to teach and to learn.
Adhesions are very difficult to treat and adhesion treatment is a challenge for the medical and scientific community. Nothing is 100 % certain, nothing is guaranteed, there is no standard treatment, no available medication guarantees success – some seemingly successful medications have even been withdrawn from the market suddenly. So we need to work together and not be distracted by the unproven remarks of a minority who unfortunately did not get the results they wished for from surgery or those who didn’t have any surgery with me at all!
Those who complain are those who normally did not get the results that they wished for. Generally, there is little feedback from the successful cases since they have resumed their normal lives and don’t have a need for patient support organisations or to post comments on message boards. This should be taken into consideration when making any comments about treatment.
I will try to explain what adhesions and adhesion surgery are. I will do this regularly, and in the context of Helen’s ARD course where I can refer to her explanations. This is, by the way, a good example of an excellent patient-doctor relationship.
1) The surgeons describe adhesions using a SCORE system: firstly by the number of adhesions (e.g. covering an area of 15 cm) and, secondly, by their severity (how they are attached to the organs, how dense, filmy, etc), and how they can be removed (sharp dissection, bloodless cutting, etc). There is much more to a surgeon’s view on adhesions than meets the eye. We see an improvement of the adhesion score as a success, whereas the patient often sees an improvement of symptoms or a complete disappearance of symptoms as a success!
2) After surgery some adhesions may return. Again, we measure this by scoring, so we might have an improvement of an adhesion situation while the patient says s(h)e has pain and therefore concludes the adhesions are back!
In some cases there may be a huge improvement of adhesions (by 90%), but some small adhesions might have formed somewhere and cause extreme pain. Small adhesions can even cause bowel obstructions (briden ileus)!
Overall, even if a surgeon reduces adhesions by 90% (as in this individual case), the patient has pain that returns and therefore considers the procedure to be a total failure (0% healed).
Do you see the difference?
Consider the following option: In the event a patient develops pain again, it would take only 30 minutes of surgery to remove this small adhesion that causes the pain. This would represent a 100% healing (100% success) using a minor procedure. That is how fine the line is between surgical success or failure!
In the follow-up many could improve their situations and we can all learn and contribute to finding better solutions to ARD problems!
3) All cases of adhesion are unique and every patient reacts differently to surgery, pain, adhesion barriers, etc, SO no conclusions can be made from one individual case. The only factors which can be taken into account are the results of the whole group under investigation. If individual outcomes would be used to gauge the success of a medical product or treatment, medical science would stagnate since there are always a few negative results, and those are the patients who tend to complain.
Our results reflect the global group and not individuals. For those who had „no success“ there is an option which I mentioned above which can lead to improved individual results.
We also have to exclude some individuals from the group. In order to assess the success rate of an adhesion treatment, we have to divide all patients who had the same treatment, the same adhesion SCORE (amount of adhesions and their severity) into small sub-groups to estimate the results and compare them to each other. We would otherwise be comparing apples to pears.
For example, patients with adhesions covering an area of about 20 cm have to be viewed together and can’t be compared to patients who have an area of 5 cm or where the entire abdomen is full of adhesions (around 50 cm of adhesions). For a correct comparison, even groups of healthy and ill patients in every sub-group would have to be assessed, and so on.
Simply put, we compare the adhesion score (number of adhesions) and the severity score of adhesions at initial surgery, with the scores in the second examination and we come to a long term follow-up. In our first protocol we include only patients with a follow-up of at least 3 months. We exclude all patients with the following criteria:
No second examination laparoscopy
Further surgery (e.g. gall bladder, appendix)
Patients with complications during initial surgery or second examination
An infection after the initial surgery (e.g. peritonitis)
2nd surgery not in our facility and without proper documentation of the previous surgery sites
Refusal of the follow-up or second-look operation.
Just to clarify a point, gall bladder surgery can also cause adhesions in the lower pelvis as there is blood that coagulates, seeping down to the lower part of the body when the patient is standing. This is how you can develop adhesions in the pelvis area after the upper organs have been operated on.
All patients with pain need to confirm that their pain is associated with a reformation of adhesions and not to any other issues like gastritis, pancreatitis, stress, individual issues and other factors. This is best done by a 3rd laparoscopy offered in our concept of adhesion treatments. These adhesions have to be well documented in images, as they might have consequences for the surgery procedure or the adhesion barrier. We offer this to our patients at no charge for the surgery itself if it is pperfromed in between of 12 weeks post initial surgery.
4) The whole peritoneum is an ORGAN that helps defend the abdominal cavity and therefore there is a permanent exchange of fluids and cells. It permanently builds new cells to prevent infections. In so doing it repairs itself, the integrity of the organ “peritoneum”.
A foreign body, like for instance your menstrual blood, causes irritation and local inflammation. Blood in general causes irritation. This is, for example, why endometriosis nearly always produces some adhesion, generally in the pelvic area and sometimes in the entire abdominal cavity. This, and surgery conducted on genital organs, is the reason why adhesions are more prevalent in women.
Infections, even slight ones, can cause inflammation, thus regenerating the peritoneum resulting in adhesions (scar tissue). This is a normal healing process. A good example is our skin. When you graze your skin after a fall, you will see how the skin heals. First it bleeds, then it forms a scab to prevent contamination with bacteria, then new skin forms under the scab and finally the scab falls off. Compared to a simple cut from a knife, this is a long healing process. Wounds covering a larger area are much more susceptible to infection and take longer to heal.
The wounded tissue after adhesiolysis is comparable with the skin healing process. And the areas are sometimes very large. The main aim of adhesion surgery is to prevent infection. Proper equipment and antibiotics might help in some cases, but usually there is always a “reaction” to surgery. In some patients this might be slight, in others severe. In some cases this process can result in adhesion formation, in others not. If the regeneration process takes 8 weeks, the patient might develop adhesions in this period. In the case of an infection, it might even take up to 16 weeks.
Surgeons cannot guarantee that adhesiolysis will succeed, but we are doing our BEST!
To estimate risk, a second laparoscopy is a good tool to determine the chance of adhesion formation. Experiments show that adhesions form in the first 7 days after surgery, so if we don’t have adhesions 7 days after the initial adhesiolysis, and the patient doesn’t get any infection or undergoes any further surgery, we can conclude that there will be no adhesions. The concept of the 3rd examination of patients who have developed pain after the second examination (in a period of 12 weeks), allows us to confirm or exclude adhesion formation and to deal with it. This will occur within the mentioned 12 week period and after the second examination. Also, within this time frame the adhesion formation will be very minor and can be easily dealt with.
The results are as follows:
All adhesion scores that were described in the literature mostly concerned genital organs and are therefore inappropriate for comparing scores of bowel adhesions. As most of our patients suffer from bowel adhesions and severe adhesion status, we developed our own score system. This will be published at a later date.
Our adhesion treatment with gasless laparoscopic adhesiolysis and SprayGel there was applied to 9 German patients and 36 from other countries. Before the availability of SprayGel we performed adhesiolysis with gasless laparoscopy but without any adhesion barrier. Of the 45 patients only 27 could be included in the tests (see exclusion criteria above).
18 patients had the following exclusion criteria:
3 because of other surgery (gall bladder, appendicitis)
5 with complications during initial surgery or second procedures or a frozen abdomen
3 because there is no follow-up.
7 with a follow-up shorter than 3 months
Of 34 patients (27 + 7 with short follow-up) = 31 patients, 91 % were adhesion free at the 2nd laparoscopy at 7 days postoperative.
Three patients had small (less than 3 cm) adhesion attachments to the incision sites at the second examination 7 days post-operatively. These were removed very easy by simply touching them with an instrument. We assume that no adhesions will recur as none of these 3 patients have developed pain in the follow-up.
Of the 27 patients, 4 developed pain after surgery, which means that 85 % of patients were free of pain 3 -13 months later.
Of the 4 patients with pain, 2 had a 3rd laparoscopy with no adhesions detected. This means that only two patients didn’t have a 3rd examination and might have adhesions (one of the patients is going to have her 3rd laparoscopy at the end of September).
Even if I assumed that these 2 remaining cases had adhesions, the adhesiolysis success rate procedure WOULD translate to 25 of 27 patients being adhesion and pain free, the equivalent of 92,6 %.
If we extrapolate this even further to include another 3 with no follow-up (exclusion criteria) who complain about pain but decided to have no follow-up, and we count them as having adhesions, it would represent only 5 of 30 patients with 83 % adhesion and pain free!
I think the results are excellent. In my opinion there is a huge difference between gasless laparoscopy compared to laparoscopic adhesiolysis with carbon dioxide!
The literature on gynaecological adhesions (NOT bowel adhesions) reports 71 % adhesion free statuses at the second stage with no long-term follow-up. Others are reporting a rate of 63 % of patients with no pain.
There is no other published research on (gasless)-laparoscopic adhesiolysis with an application of an adhesion barrier and a second laparoscopy with regard to severe bowel adhesions.
One should bear in mind that even very difficult cases which require more than one procedure to achieve an improvement in adhesion formation end up being better than before surgery. One could CREDIT our treatment as an enormous improvement, considering that no other surgeon would even think of operating on this patient.
——————–
Dr. med. Daniel Kruschinski
Gynäkologische Adhäsiolyse
Die meisten unserer Verwachsungslösungen (Adhäsiolyse) betreffen Darmverwachsungen.
Hier ist ein Fall mit gynäkologischen Adhäsionen, die einen Einfluss auf die Fertilität haben können oder Schmerzen verursachen.
Die linke Beckenwand is komplett mit Darm zugewachsen. Man kann lediglich die Spitze des linken Eierstocks (weiss) erkennen:
Nach durchgeführter lift-laparoskopischer Verwachsungslösung kann die weibliche Anatomie sehr gut erkannt werden:
linker Eierstock und linker Eileiter mit Fimbrienende.
Der Darm liegt an seiner korrekten anatomischen Position.
Applikation von Spraygel als Verwachsungsbarriere …

und in der Second-look Bauchspiegelung: keine Neubildung oder Reformation von Verwachsungen.

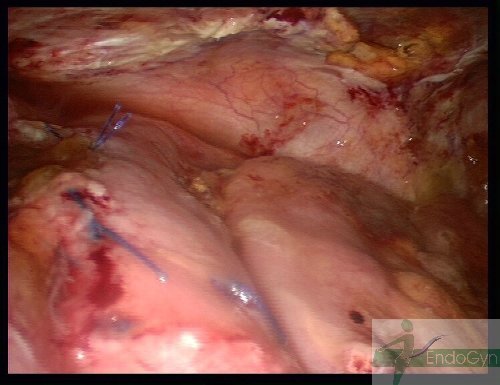
Ausgeprägter Verwachsungsbauchbauch
Lift-Laparoskopie und SprayGel funktionieren zusammen sogar in den schlimmsten Fällen, wo fast der gesamte Bauch mit
Verwachsungen ausgefüllt ist: und der Darm mit seiner ganzen Wand komplett and die Bauchdecke angewachsen ist,
so dass die Lösung dieser Darmanteile imme sehr gefährlich ist:

weil der Darm verletzt werden kann…und genäht werden muss:
Applikation von SprayGel als Verwachsungsbarriere:
und in der Second look Laparoskopie: der Darm ist optimal verheilt, die Nähte halten sufficient,
keine Infektionen oder Reformation von Verwachsungen:
Massive Verwachsungen
Eine Patientin aus Deutschland mit massiven Verwachsungen und ihre Second-look-Laparoskopie.
Das sind Bilder vor der Verwachsungslösung:
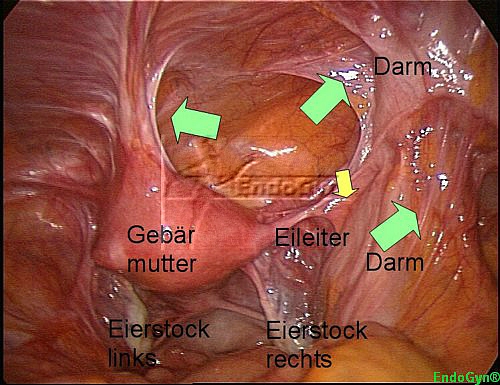
Die Gebärmutter hängt derb in der vorderen Bauchdecke bei Zustand nach einem Kaiserschnitt in Indien.
Der Darm rechts hängt ebenso fest in der Bauchdecke, der rechte Eileiter ist komplett mit Darm verwachsen und nicht zu sehen.
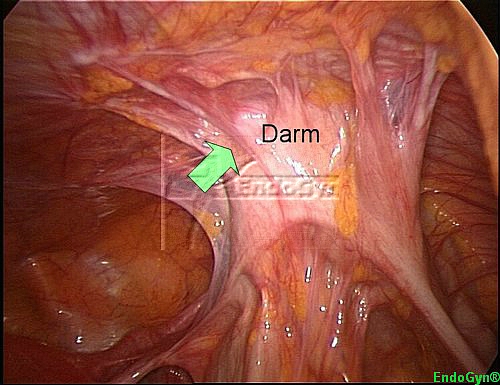
Auf diesem Bild kann man erkennen, wie derb der Darm in der Bauchdecke festhängt.
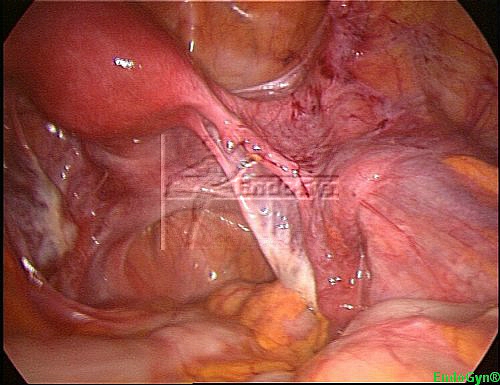
Nach der Verwachsungslösung ist der Eileiter komplett frei…
und der Darm komplett aus der Bauchdecke herausgelöst.
Auch die Gebärmutter ist aus der Bauchdecke herauspräpariert und beweglich (war vorher fixiert).

Applikation von SprayGel über das chirurgische Feld…
und keine Verwachsungen in der Second-look-Laparoskopie
nicht zwischen Darm und Bauchwand
und nicht zwischen Gebärmutter und Bauchdecke.

Auch der Eileiter ist komplett frei und wir dürfen hoffen, das nächste SprayGel Wunder Baby bald begrüßen zu dürfen !
Verwachsungen künstl. Netz I
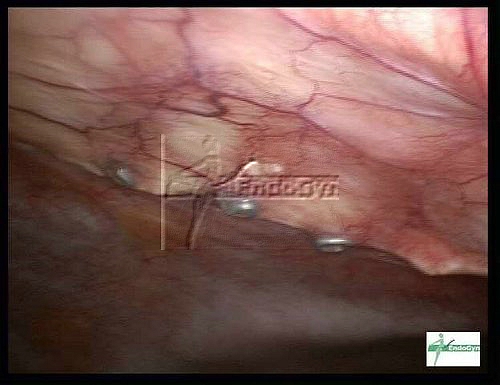
Wenn ein sog. künstliches MESH eingesetzt wird, z.B. für den Verschluss von Bruchpforten oder wie in diesem Fall für die
Stabilisierung eines TRAM-Flap (Brust Rekonstruktion mit dem Transversus abdominis Rektus Bauchmuskel), können sich
Verwachsungen zu diesem MESH bilden.
Diese Patientin aus Texas / USA wurde von Ihrem Chirurgen schon 4 mal operiert und die Verwachsungen kamen immer wieder.
Der Chirurg und seine OP-Schwester haben übrigens die Patientin zur Chirurgie nach Deutschland begleitet, um sich die
Verwachsungslösung bei uns anzuschauen.
Hier sind die Bilder:
Man erkennt das MESH Material, unter welchem sich die Verwachsungen gebildet haben.
Nach Lösen der Verwachsungen wurde SprayGel appliziert

in der Second look Laparoskopie sind keine Verwachsungen mehr zu sehen.

Und bei der gleichen Patientin, die eine Gebärmutterentfernung mit Bauschschnitt vor Jahren hatte, haben sich auch
Verwachsungen im unteren Bauch gebildet.
Hier sind Verwachsungen zur linken Beckenwand, die am Darm zweifach extrem ziehen.
und nach Lösen dieser Verwachsungen
wurde SprayGel appliziert
und in der Second-look Laparoskopie haben sich in diesem Bereich keine Verwachsungen mehr gebildet.
Verwachsungen künstl. Netz II
Eine Patientin aus den USA hatte 23 Vor-Operationen.
Als letzte Operation wurden Brüche in der Buchdecke durch ein künstliches Mesh stabilisiert.
Mesh als Fremdmaterial bewirkt natürlich massive Verwachsungen um das Mesh herum (Bild 1) und insbesondere um die
Metalllschrauben, die zur Fixierung eingesetzt wurden (Bild 2 und 3). Die Oberfläche der Leber war ebenfalls in diese
Verwachsungen involviert (Bild 4). Das Bild Nr. 5 zeigt das Endresultat nach Verwachsungslösung. Die Metallscharauben wurden
mit Fettgewebe abgedeckt gelassen, um evtl. neue Verwachsungen zu verhindern.
Bild 1 
Bild 2 
Bild 3 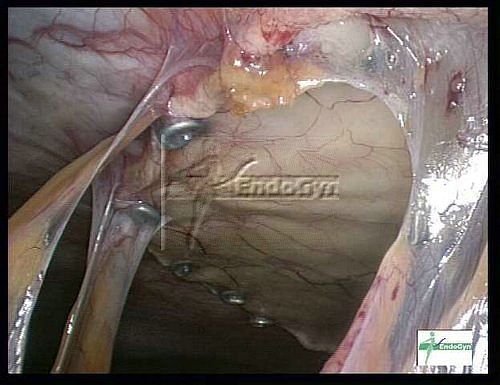
Bild 4
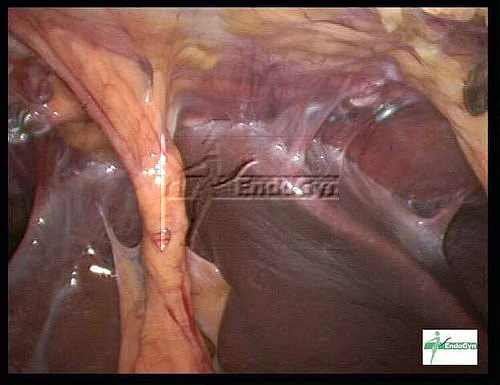
Bild 5 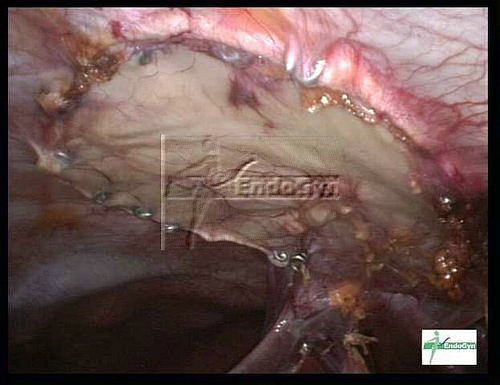
Im second look zeigte sich ein gutes Resultat: keine Verwachsungen im Meshbereich und auch keine Verwachsungen
zu den Metallschrauben, die schön mit Fett abgedeckt sind.
Die neue Technik, die Schrauben mit Fettgewebe abzudecken hat funktioniert.


Chirurgie, die nichts bringt
![]()
und die Patienten in Gefahr bringt, denn eine Operation, speziell bei Verwachsungen kann sehr gefährlich sein !
Nachfolgende Bilder zeigen. warum z.B. eine chirurgische Entfernung von Verwachsungen ohne anschließende Behandlung mit sog. Barrieresubstanzen, wie z.B. SprayGel und ist absolut unnötig und sinnlos.
Diese Patientin hat Verwachsungen zwischen Darm / linker Beckenwand / Gebärmutter.


Nach 4 Stunden Chirurgie sind alle Organe präpariert und anatomisch optimal wiederhergestellt:

Wegen einer kleinen Serosaeröffnung des Darmes, die genäht ist, gaben wir kein SprayGel (Verwachsungen-Barriere) in der ersten Sitzung, damit eine mögliche Infektion, die auftreten könnte, nicht verstärkt wird. In solchen Fällen machen wir die sog. Second-look laparoskopie ca. 4-5 Tage nach dem Ersteingriff und bei intakten Verhältnissen applizieren dann das SprayGel / SprayShield.
Und schauen Sie bitte, welchen Effekt eine Verwachsungschirurgie ohne SprayGel hat:

In diesem und einigen anderen Fällen, in denen das SprayGel nicht appliziert wurde, konnten wir die Realität sehen: eine Verwachsungsoperation ohne SprayShield / SprayGel ist in den meisten Fällen erfolglos !!!

Die Verwachsungen haben sich alle zurückgebildet und sind sogar schlimmer …
und wenn die Patienitin nicht in unserem Konzept der Verwachsungsoperationen stünde, wäre all die Arbeit und Mühe der Operation ohne Ergebniss und hätte nur zufolge, dass eine Operation ohne Effekt, aber mit erhöhten Komplikationensmöglichkeiten für die Patientin resultiert hätte…
Wegen der frühen Second-look Laparoskopie in den Fällen, wo der Darm verletzt war, sind die Verwachsungen nur gerade angelegt und können mit einem Instrument durch einen leichten Druck, ohne Blutungen, gelöst werden:

In unserem Konzept der Chirurgie von Verwachsungen ist es möglich, den Darm zu überprüfen (er war intakt in diesem Fall) und SprayShield / SprayGel zu applizieren, welches sicher die Bildung von Verwachsungen verhindern wird.

Ohne der Verwachsungsbarriere SprayShield / SprayGel und ohne einer SECOND-LOOK LAPAROSKOPIE wäre diese Chirurgie unnötig und gefährlich !
Bitte achten Sie darauf, dass Sie im Falle von Verwachsungen NICHT mit Bauchschnitt und NICHT OHNE Barriereseubstanzen (am besten SprayShield) und NICHT OHNE einer second-look Bauchspiegelung (möglichst ohne Gas) operiert werden.
Es ist auch wichtig, sich von einem auf Verwachsungen speziallisierten Chirurgen operieren zu lassen, der ein Konzept und eine Infrastruktur für Verwachsungsoperationen hat und Sie nicht nach einem Tag oder sogar ambulant nach Hause schickt, sondern seine Operation per second-look Laparoskopie überprüft !
Erfolglose Operationen mit Kohlendioxid-Gas
Bitte beim Thema oben anschauen, was passiert, wenn Chirurgen keine Adhäsionsbarrieren einsetzen…
Aber auch, wenn die beste Adhäsionsbarriere eingesetzt wird, aber mit Kohlendioxid – Gas, ist die Chirurgie in den meisten Fällen wirkungslos und unnötig.
Dieses Bild zeigt die Wundfläche nach einer langen Vrewachsungslösung mit CO2 – Gas:

nach Einsetzen des SprayShield / SprayGel sieht man, dass es nur an einigen Punkten haftet, aber nicht die gesamte Wundfläche abdeckt.
Ja es gleitet sogar nach unten weg ! Das passiert, da das Bauchfell durch das CO2 sauer und sauerstoffarm ist.

Und hier ist eine ähnliche Fläche aus einer gaslosen laparoskopischen Verwachsungslösung…

und nach Abdecken mit SprayShield / SprayGel !
Vergleichen Sie bitte oben mit der abgedeckten Fläche beim Einsatz der Laparoskopie mit Gas…

Kommentar: der schmale Spraystrahl beim Einsatz in der Gas-Laparoskopie verhindert die Abdeckung großer Flächen,
d.h. ein kit SprayShield / SprayGel deckt kleinere Flächen ab als unter der gaslosen Methode (also MEHR Kosten).
Das SprayShield / SprayGel klebt an einzelnen Punkten, bedeckt aber nicht die gesamte Wundfläche gleichmäßig.
Meiner Meinung nach geschieht dies, weil der Gasdruck verhindert, dass sich das SprayShield / SprayGel
richitg mit Luft vermischt und kleinste Sprühpartikel bildet UND durch das saure und sauerstoffarme Bauchfell wird
das SprayShield / SprayGel gar nicht aufgenommen !!!
Folgerung: Nach meiner persönlichen Meinung ist das enorm wichtige Abdecken der Wundfläche
mit SprayShield / SprayGel am besten unter dem Einsatz der gaslosen Laparoskopie möglich.
Vornehmlich sollte die Zeit der Anwendung von CO2-Gas auf unter 2 Stunden verkürzt werden,
um spätestens dann auf die gaslose Lift-Laparoskopie bei der Operation von Verwachsungen zu wechseln.
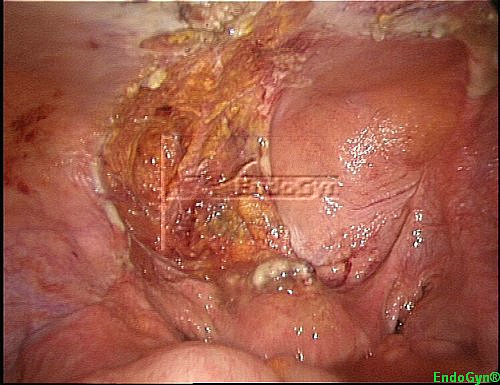
Patient I
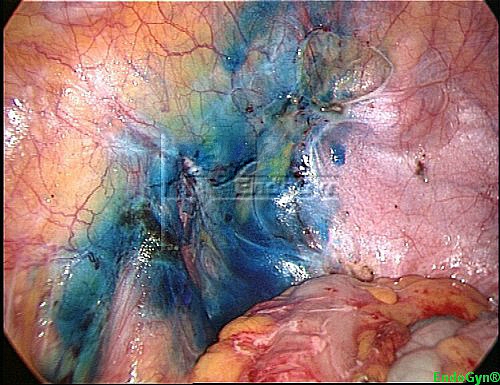
Left pelvic and abdominal wall adhesions
 |
 |
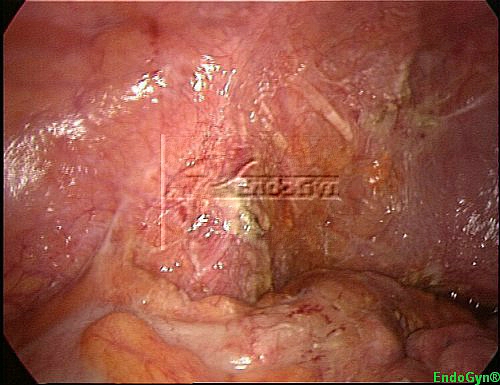
| Left pelvic brim and anterior abdominal wall, omental and bowel adhesions | Another view to show the bowel involvement |
 |
 |
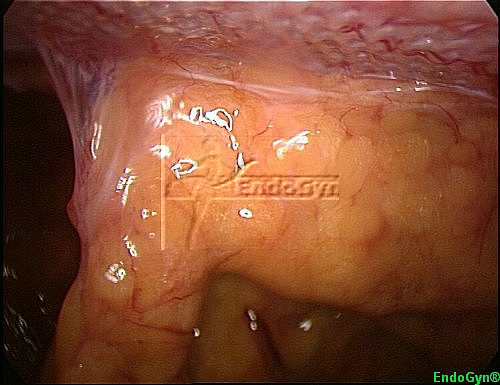
| After first dissection of adhesions, bowel involvement | The left pelvic brim and the anterior abdominal wall after dissecting the adhesions |
 |
 |
| The left pelvic brim and the anterior abdominal after application of SprayGel™ | The left pelvic brim and the anterior abdominal at the second-look laparoscopy on day 7 postoperative |
Your content goes here. Edit or remove this text inline or in the module Content settings. You can also style every aspect of this content in the module Design settings and even apply custom CSS to this text in the module Advanced settings.
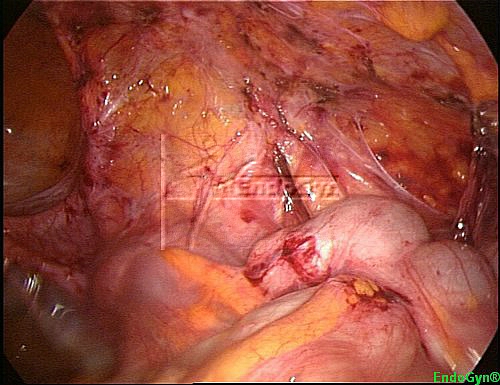
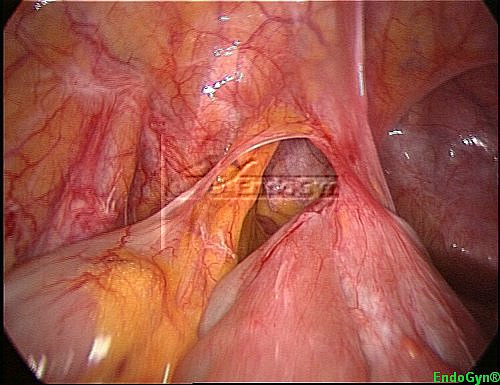
Left pelvic wall adhesions (including 3rd-look laparoscopy)
 |
 |
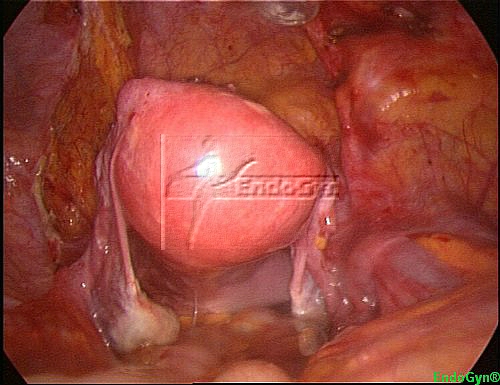
| Left pelvic brim with big bowel adhesions | Left pelvic brim after adhesiolysis |
 |
 |
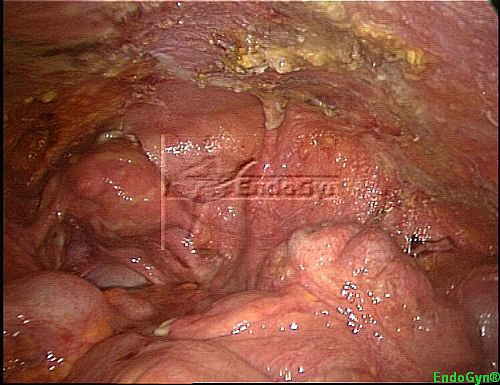
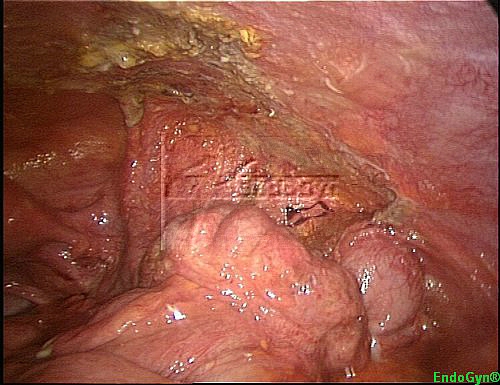
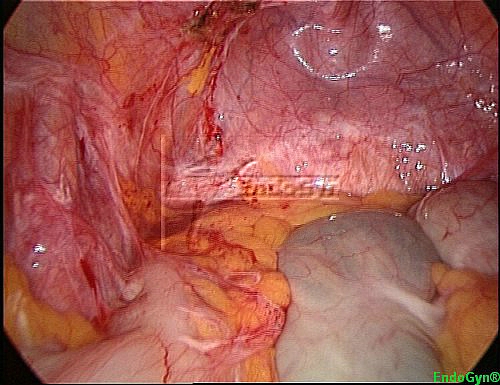
| Left pelvic brim after application of SprayGel™ | Left pelvic brim at the second-look laparoscopy (on day 7 postoperative) |
 |
|
| Left pelvic brim at 3rd-look laparoscopy 12 weeks after initial adhesiolysis |
Right upper quadrant adhesions(including 3rd-look laparoscopy)
 |
 |
| Adhesion in the right upper quadrant | Another view of the adhesion in the right upper quadrant showing how the big bowel is involved and twisted |
 |
 |
| Right upper quadrant after adhesiolysis | Right upper quadrant after adhesiolysis |
 |
 |
| Right upper quadrant at the second-look laparoscopy | Right upper quadrant after the 3rd-look laparoscopy 12 weeks after initial adhesiolysis |
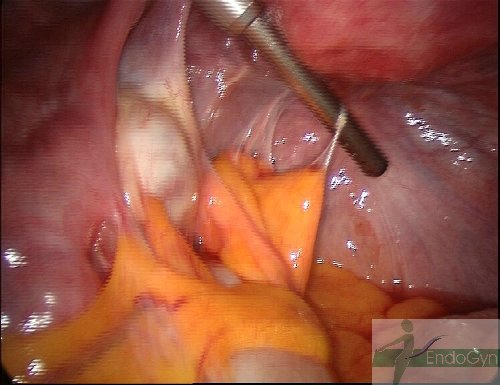
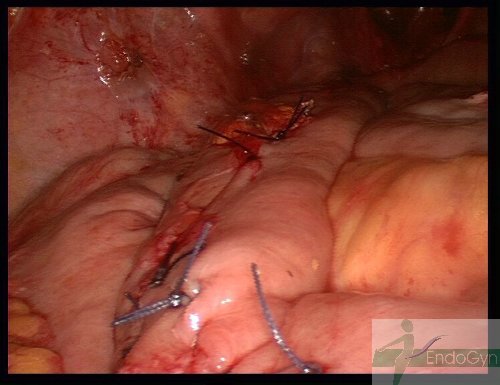
Midline bowel to abdominal wall adhesions
 |
 |
| Midline adhesions of the small bowel to the anterior abdominal wall | Another view of the adhesions and the bowel loops and the abdominal wall |
 |
 |
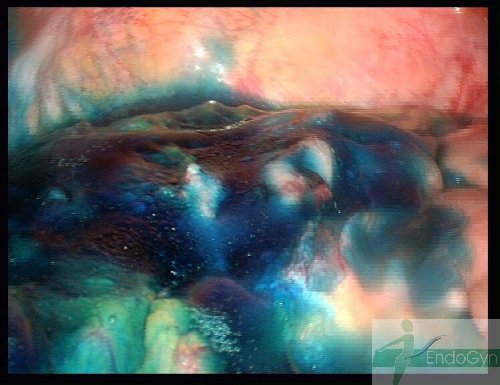
| During the adhesiolysis, please notice how near to the bowel serosa we need to cut, and even then there’s no lesion with our special equipment | After the adhesiolysis SprayGel™ has to be applied on the abdominal wall and … |
 |
 |
| … on the bowel surface at the wounded area | The abdominal wall at the second-look laparoscopy, only scar tissue and no adhesions |
 |
 |
| Second-look: the bowel area which already has healed-up completely, the new vessels (Neoangiogenesis) in the wounded area helped the healing process with a better blood and oxygen supply |
Right middle and upper quadrant adhesions
 |
 |
| Adhesions in the right middle and upper quadrant, involving big and small bowel | Another view of the adhesions and the liver and bowel involvement |
 |
 |
| Here one can see how the liver is pulled by a dense adhesion … | … and how the bowel is pulled by the adhesions |
 |
 |
| The right middle and upper quadrant after adhesiolysis | The right middle and upper quadrant after adhesiolysis and application of SprayGel™ |
 |
 |
| Second-look laparoscopy: the adhesiolysis area has healed-up and the SprayGel™ covered new peritoneum grew over the wounded issue | Second-look laparoscopy: also the liver is now free of adhesions |
Left abdominal wall adhesions
 |
 |
| Adhesions in the left middle and lower quadrant, involving big bowel | Another view of the adhesions and a twisted bowel loop that was involved in the adhesions |
 |
 |
| Another view of the adhesions and a twisted bowel loop that was involved in the adhesions | The left lower quadrant after adhesiolysis and application of SprayGel™ |
 |
|
| Second-look laparoscopy: The adhesiolysis area and SprayGel™ covering this area |
Left abdominal wall adhesions
 |
 |
| Left anterior abdominal wall, omental and bowel adhesions | The omentum is completely adherent to the abdominal wall |
 |
 |
| The left anterior abdominal wall after dissecting the adhesions | The left anterior abdominal wall after complete adhesiolysis |
 |
 |
| The left anterior abdominal after application of SprayGel™ | The bowel area opposite to the anterior abdominal after application of SprayGel™ |
 |
 |
| The anterior abdominal wall after Second-look laparoscopy on day 7 postoperative | The anterior abdominal wall after Second-look laparoscopy on day 7 postoperative |
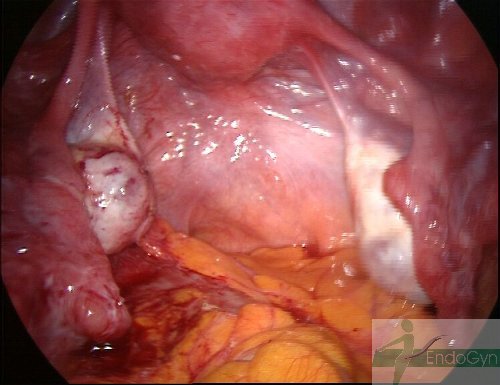
Right pelvic wall adhesions
 |
 |
| Right pelvic wall, bowel adhesions | Right pelvic wall, the bowel is completely adherent to the pelvic wall |
 |
 |
| Right pelvic wall after complete adhesiolysis, left the ovary can be recognized | The pelvic area after application of SprayGel™ |
 |
|
| The pelvic area at the second-look laparoscopy at day 7 postoperative, left one can see the ovary |
Midline and left abdominal wall bowel adhesions
 |
 |
| Midline and left anterior abdominal wall bowel adhesions | Another view on the abdominal wall bowel adhesions, many loops are attached to the abdominal |
 |
 |
| The abdominal wall after dissection of the bowel adhesions, on the right one can see the diathermic scissors | The abdominal wall after dissection of the bowel adhesions |
 |
 |
| The abdominal wall after dissection and after application of SprayGel™ | The anterior abdominal wall at the second-look laparoscopy at day 7 postoperative |
 |
 |
| The anterior abdominal wall at the second-look laparoscopy at day 7 postoperative, the white spots are representing the forming scar tissue | The peritoneum at the second-look laparoscopy shows neoangiogenesis (new vessels growing) which allows more blood and oxygen supply to the wounded area |
Upper right quadrant bowel adhesions
 |
 |
| Upper right quadrant adhesions | Another view of the bowel adhesions, many loops are attached together |
 |
 |
| Bowel adhesions during adhesiolysis which frees every loop out of the conglomerate | The right upper quadrant after dissection of the bowel adhesions |
 |
 |
| The right upper quadrant after dissection of the bowel adhesions and application of SprayGel™ | The right upper quadrant at the second-look laparoscopy at day 7 postoperative |
 |
 |
| Another view of the right upper quadrant at the second-look laparoscopy at day 7 postoperative | The peritoneum at the second-look laparoscopy shows neoangiogenesis (new vessels growing) and forming of white scar tissue |
Right upper quadrant adhesions
 |
 |
| Severe adhesions between small bowel and right abdominal wall | The same area after dissecting the adhesions |
 |
 |
| After application of SprayGel™ | At the second-look laparoscopy |
 |
|
| The same area after 12 weeks at the 3rd-look laparoscopy, the healing of the peritoneum resulted in white scars, but without adhesions |
